The conversation in Australia is slowly changing when it comes to both understanding and acknowledging adverse health effects in susceptible individuals from innate immune activation following exposure to indoor dampness and mould. Some of the science around this topic is new, which means even many working in the healthcare system are not yet aware of it. As such, Toxic Mould Support Australia (TMSA)—the country’s primary patient support group for those suffering from Chronic Inflammatory Response Syndrome (CIRS)—would like to play a role in educating Australians on this health issue by offering a package of relevant reports and peer-reviewed studies. For anybody needing to put critical information for their healthcare in the hands of their medical practitioners, this primer provides a summary of two Australian Government reports, one WHO report, and ten peer-reviewed scientific publications.
Relevant Australian Government and WHO Reports
Following federal MP Lucy Wicks falling sick with CIRS in 2015, the Australian Government conducted an inquiry into biotoxin-related illnesses in Australia. The inquiry tabled responses from affected individuals, researchers, indoor environmental professionals, clinicians, and the Department of Health. Following this, the Australian Government published a report containing seven recommendations regarding how Australia should proceed with regards to those affected by biotoxin-related illnesses.
Several of the committee’s relevant recommendations were:
1. The Department of Health produce and publish in the short term a fact sheet, and in the medium term undertake further research on the potential health effects of exposure to damp and mould; the prevalence of dampness and mould in the built environment; and advice on the prevention and removal of mould.
[Recommendations 2-4 were concerned with the building/environmental side]
5. The Department of Health conduct a review into the treatment of patients presenting with complex illnesses that are difficult to diagnose such as those with CIRS-like symptoms.
6. The Australian Government commission the National Health and Medical Research Council to conduct research into CIRS-like syndromes with a view to assisting in the diagnosis, treatment and management of patients. Research should also examine any links between mould and biotoxins and complex symptoms most commonly reported as typifying CIRS.
7. The Department of Health, in consultation with patient groups, medical practitioners, and health bodies, develop clinical guidelines for general practitioners for the diagnosis, treatment and management of CIRS-like conditions.
In 2020, the Australian Government published a paper detailing their proposed responses to these recommendations.
As part of the Australian Government’s response to the 2018 Inquiry into Biotoxin-Related Illnesses, the National Health and Medical Research Council (NHMRC) published a consultation paper on biotoxin-related illnesses in Australia. As part of this paper, they conducted an initial literature review in which they stated:
“While the Committee heard there was insufficient evidence and a lack of consensus in Australia on the potential health impacts of biotoxins associated with mould and water-damaged buildings, a number of predominately international studies have reported a range of possible health effects and point to a growing body of evidence in this area.”
More specifically, they noted in the literature:
“… associations between living in water-damaged buildings and adverse health effects including CIRS-like symptoms. These symptoms can include ongoing fatigue, headaches, pain, eye problems, gastrointestinal tract problems, cognitive symptoms such as ‘brain fog’, skin issues and muscle cramps, amongst others.”
The report also notes that approximately one in every ten Australians occupy housing ‘likely to adversely impact their health’, and that this problem disproportionately affects those who already suffer other forms of disadvantage.
The NHMRC allocated $1,063,797 of funding as part of a targeted call for research in this area to the following study:
An Integrated Biomarker Platform for the Early Diagnosis and Treatment of Chronic Inflammatory Response Syndrome in Australia.
WHO found sufficient epidemiological evidence across different countries and climates that occupants of damp or mouldy buildings are at increased risk of respiratory symptoms, respiratory infections and exacerbation of asthma. Some evidence suggested increased risks of allergic rhinitis and asthma.
In addition, while many in medicine are not aware of dampness and mould causing immunological effects, WHO explicitly noted this:
“Exposure to microbial contaminants is clinically associated with respiratory symptoms, allergies, asthma and immunological reactions.”
Such effects can occur in water-damaged buildings:
“Toxicological evidence obtained in vivo and in vitro supports these findings, showing the occurrence of diverse inflammatory and toxic responses after exposure to microorganisms isolated from damp buildings, including their spores, metabolites and components”.
Damp buildings can also suppress immune responses:
“The immunosuppressive effects of mycotoxins have been confirmed in experimental animals. Trichothecenes T-2 and deoxynivalenol (vomitoxin) impair immune responses to respiratory virus infection, increasing the severity of infection.”
These effects are not purely from mycotoxins:
“The acute cytotoxicity of fungal strains in damp buildings has been found to be due to the metabolite profile produced in vitro, although their biological activity may not depend solely on toxin production. Fungal spores appear to have toxic effects other than those that cause the inflammatory reaction.”
Finally, they clearly noted mechanisms of injury in categories beyond the more established and accepted allergy, infection, and toxic effects of exposure to dampness and mould:
“Mechanisms of injury include exposure to β-glucans, toxins, spores, cell fragments and chemicals followed by immune stimulation, suppression and autoimmunity as well as neurotoxic effects.”
WHO also noted the difficulty in understanding such effects:
“The synergistic interactions among microbial agents present in damp buildings suggest that the immunotoxic effects of the fungal and bacterial strains typically found can be potentiated during concomitant exposure, leading, for instance, to increased cell death or cytotoxic or inflammatory effects. Such interactions can give rise to unexpected responses, even at low concentrations of microbial (or chemical) agents, so that it is difficult to detect and implicate specific exposures in the causation of damp building-associated adverse health effects.”
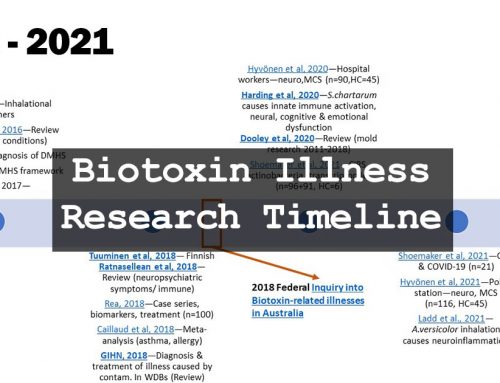
Ten Relevant Peer-Reviewed Studies
This double-blind, placebo-controlled trial elegantly showed cause-and-effect of inhaled mould, with and without mycotoxins. They administered Stachybotrys chartarum spores intranasally to mice in three groups:
- Mice administered a placebo (saline);
- Mice administered Stachybotrys spores; and
- Mice administered Stachybotrys spores denatured of their mycotoxins.
Harding et al found innate immune system activation, neuroinflammation, neural and behavioural problems, systemic inflammation, and pain. As per their discussion:
“There is now compelling evidence that mold exposure causes serious multi-system health problems in humans including peripheral immune activation and behavioral dysregulation that implies central effects.”
Effects are more likely to occur in genetically susceptible individuals and can have severe consequences:
“… roughly 25% of Americans carry major histocompatibility complex gene variants that make them susceptible to long-term inflammation following mold exposure, including the initiation of autoimmune problems and changes in brain structure/function…”
As WHO noted, the effects are not simply from mycotoxins but the spores themselves:
“Our data document for the first time that exposure to known quantities of both toxic and non-toxic mold spores activated a central neural immune response with concomitant cognitive and emotional dysfunction. In addition, we identified a mechanism, innate immune activation, which aptly explains how mold exposure may cause such a diverse array of problems.”
Related: Recently, a different group of US researchers (Ladd et al., 2021, ASN neuro) found that Aspergillus versicolor inhalation in mice negatively altered gene expression of neuroinflammatory, glial activation, and neurotransmitter pathways.
“Here, we demonstrate that a moderate A. versicolor exposure, the most common opportunistic filamentous fungal species in damp indoor environments, triggers neuroinflammation gene expression with short term exposures (1 and 2 weeks) in multiple brain regions.”
This research showed that the tested species (A. versicolor) differed in effects from what Harding et al.’s research showed using Stachybotrys chartarum. One example is that exposure to A. versicolor did not lead to either cell death or toxicity to developing neurons in the hippocampus.
This systematic review considered 114 epidemiological studies concerning human exposure to indoor microbial growth between 2011 and 2018. The combined total number of participants was 270,454 across 30 countries and 5 continents.
Notably, the vast majority of published studies found adverse health effects from dampness and mould:
“The proposition that inhaled mold, mold fragments, toxins and inflammagens, or other components of the air in WDB, cause single and multi-system illness, is supported by 112 of 114 (98.2%) epidemiological articles published between 2011 and 2018.”
This doesn’t exclude the possibility of publication bias. However, it should be noted that, just as WHO found in their 2009 review, studies from the subsequent decade also support immunological and neurological effects:
“One hundred reports further supported previous works regarding respiratory, and 60 supported immunological effects. Twenty-four supported general adverse health effects and 16 studies supported cognitive decline.”
Notably, the included studies found statistically significant symptoms in systems not typically associated with dampness and mould, such as neurological, immunologic (allergic and non-IgE mediated), cognitive, and ophthalmologic.
This review incorporated 16 prior studies on the adverse effects of inhaled mould and mycotoxins in indoor environments and concluded:
“Individuals exposed to mold report an extensive range of symptoms, including malaise, fatigue, and cognitive impairment, which appear to be related to the duration of exposure.”
The authors noted that individuals exposed to moulds and mycotoxins had “symptoms affecting multiple organs, including the lungs, musculoskeletal system, as well as the central and peripheral nervous systems” and also referenced more recent evidence implicating mycotoxins in the “pathogenesis of autism-spectrum disorder”. Depression was another common symptom.
Neurological symptoms could be quantitively measured:
“…mold-exposed groups had altered neurologic functioning, including changes in body-balance, blink-reflex latency, visual fields, reaction time, and color discrimination, compared with controls.”
The mechanisms of injury involved immune effects, specifically those centred around neurological pathways such as pro-inflammatory responses mediated by cytokines from mast cells in the brain and elsewhere.
Dr Shoemaker’s landmark study of CIRS, then called Sick Building Syndrome, examined 26 patients with visible evidence of water damage and/or amplified fungal growth in their homes. The researchers compared diagnostic markers (symptom clusters, MMP-9, VCS, VEGF, MSH, IgE) against normal values. A subset of those patients (14) were included in a double-blind, placebo-controlled clinical trial that used the intervention of cholestyramine (CSM), which improved symptoms and visual-contrast sensitivity in those receiving the active intervention but not the placebo.
“These results supported the confirmatory hypotheses, thereby supporting the general hypothesis that [Sick Building Syndrome] is associated with exposure to [Water-Damaged Buildings].”
However, treatment did not lead to complete recovery:
“CSM markedly increases the elimination rate of a variety of biotoxins, but does not directly dampen the pro-inflammatory cytokine cascade initiated by exposure.”
Numerous studies now suggest dampness and mould play a relevant role in Sick Building Syndrome.
The Shoemaker-led team undertook another clinical trial of 20 patients diagnosed with CIRS caused by exposure to water-damaged buildings, refractory to previous treatment, using the compounded medication vasoactive intestinal polypeptide (VIP) with positive effects on immune dysfunction.
“Subsequent identification of correction of T-regulatory cell levels supports the potential role of VIP in both innate and adaptive immune function.”
They also found VIP:
- reduced refractory symptoms to equal controls;
- corrected inflammatory parameters C4a, TGF beta-1, VEGF, MMP9;
- corrected oestradiol, testosterone and 25-OH Vitamin D;
- returned pulmonary artery systolic pressure (PASP) during exercise to normal; and
- enhanced quality of life in 100% of trial patients.
A subsequent study by the same team (Shoemaker et al., 2017, Internal Medicine Review) showed that VIP can correct structural abnormalities in the brain caused by CIRS, as detected by volumetric MRI (NeuroQuant).
Inflammatory chronic illness due to mould and water-damaged buildings has also been investigated in Finland, where it is labelled as Dampness and Mold Hypersensitivity Syndrome (DMHS).
Daschner presented a hypothesis where the presented evolutionary analysis seeks for the ultimate causes of the vast array of symptoms in DMHS. Symptoms can be interpreted as induced by direct (toxic) actions of spores, mycotoxins, or other fungal metabolites, or on the other side by the host-initiated response, which aims to counterbalance and fight off potentially deleterious effects or fungal infection. Individual susceptibility of immune reactions can confer an exaggerated response, and magnified symptoms are then explained in terms of immunopathology.
“I show some evidence that symptoms and disease in DMHS are associated with an elevated inflammatory status, but the observed respiratory and extra-respiratory syndromes are elicited by different mechanisms, ranging from IgE-mediated allergy to multisystem, autoimmune phenomena, as well as neurobehavioral components.”
Valtonen reviewed the clinical evidence for DMHS and suggested that, given the lack of accepted laboratory tests, five clinical criteria could be used to diagnose the syndrome:
- a history of mould exposure in water-damaged buildings;
- increased morbidity to due infections;
- sick building syndrome;
- multiple chemical sensitivity; and
- enhanced scent sensitivity.
Valtonen noted that a previous study from outside of the Shoemaker team (Gray et al., 2003, Archives of Environmental Health) has also suggested a link between susceptibility to mould and Human Leukocyte Antigen (HLA) genes:
“Support for the important role of HLA genes is the fact that activated T cells (CD3+ CD26+ cells) and the class II major histocompatibility molecule MHC (CD3+ HLA-DR+) are found in over 90% of the mold exposed individuals when compared to the controls. Missing HLA genes or a deficiency in function of these genes represent a further risk in those individuals who are mold exposed.”
DMHS continues to be investigated by a number of Nordic researchers.
Bredesen, a notable neurodegenerative researcher, identified three major sub-groups of patients with Alzheimer’s Disease:
- Type 1 usually possessed the APOE-4 gene and had systemic inflammatory disorders.
- Type 2 also possessed the APOE-4 gene but typically presented with hormonal and nutritional deficiencies.
- Type 3 were more often APOE-3/3 and had disorders associated with exposures to toxins, including heavy metals, industrial toxicants, and biotoxins produced by microbial agents in water-damaged buildings.
Type 3 cases often presented at younger ages and without the common family history associated with Alzheimer’s. Symptoms were not so much amnestic as cortical, often characterised by “dyscalculia, aphasia, executive dysfunction, or other cortical deficits”.
Bredesen noted the previous research by R.C. Shoemaker and colleagues in identifying, diagnosing, and treating CIRS, a dysfunction of the innate immune system caused by a genetic inability to produce antibodies to biotoxins. This autoimmune disorder has also been identified by Nordic researchers under the DMHS moniker.
Based on previous descriptions of Alzheimer’s patients with a similar presentation, Bredesen estimated ten per cent of Alzheimer’s patients might suffer from CIRS, and then suggested why this “potential epidemic may have gone unrecognized to date” is, in part, due to a lack of broader recognition of CIRS.
“These findings suggest that patients with presentations compatible with type-3 Alzheimer’s disease should be evaluated for CIRS (as well as other toxic exposures, such as mercury and copper).”
This study was part of a broader longitudinal investigation into the health effects of various forms of indoor and outdoor air pollution on infants and children. It sought to examine the potential for mould to affect cognitive development in young children. The researchers followed a cohort of 277 babies born at term in Krakow, Poland, monitoring the presence of “visible mould patches on indoor walls” regularly between gestation and up to age 5.
A Wechsler Intelligence Scale for Children (WISC-R) was administered to the children at age six. The IQ scores of the children were adjusted for known confounders, such as “maternal education, the child’s gender, breastfeeding practices in infancy, the presence of older siblings and the prenatal exposure to lead and environmental tobacco smoke (ETS)”.
Those children exposed to indoor mould in their home for greater than two years tested with IQs an average of 10 points lower than those who had no exposure. Long-term mould exposure tripled the risk of low-IQ scoring. Moreover, the study showed that:
“… the negative effect of indoor molds on children’s IQ was consistent and stable at each level of maternal education, which is a good proxy for maternal cognitive capacity.”
This study provided additional evidence for the relationship between dampness/mould and adverse health effects but doesn’t prove causality given that examining for visible patches of mould is not conclusive of exposure to a water-damaged building.
However, this study should be considered in the context of three similar studies:
- Mustonen et al. (2016). Moisture damage in home associates with systemic inflammation in children. Indoor Air, 26(3), 439–447.
- Casas et al. (2013). Early life exposures to home dampness, pet ownership and farm animal contact and neuropsychological development in 4 year old children: a prospective birth cohort study. International journal of hygiene and environmental health, 216(6), 690–697.
- Dockx et al. (2023). Association of indoor dust microbiota with cognitive function and behavior in preschool-aged children. Microbiome, 11(1), 1.
These and several other studies curated on TMSA’s website suggest dampness and mould may play a detrimental effect on the neurodevelopment of children.
Previously, theoretical models of mould inhalation suggested that the number of airborne spores in even water-damaged buildings would not be enough to be harmful. Moreover, several studies “have shown that the concentrations of airborne fungal spores in mould problem buildings are not necessarily higher than in non-problem ones”. Admittedly, previous researchers also did not know what number of spores would be needed to cause harm, given people who were potentially exposed for long durations without ill effects, nor which moulds, other microorganisms or biotoxins might cause health problems.
Prior lab testing had predicted that spore fragments (as opposed to whole spores) might also be relevant to human health effects. These studies recognised that:
- fragments have more surface area to carry mycotoxins than whole spores;
- total exposure might be 500x higher when spore fragments are included; and
- the number of spores and fragments do not always correlate to each other.
Their results showed that the level of spore fragments was between 1,000x and 1,000,000x higher than the number of whole spores. They also noted that whole spores such as Stachybotrys chartarum can be heavy due to their water weight and settle to the floor quite quickly. Fragments, in comparison, can be ultra-fine (<0.1 μm) and stay in the air far longer.
This study disproved previous earlier theoretical models that suggested exposure levels to mould spores in water-damaged buildings were too low to cause adverse health effects.
“High particle surface area may further facilitate the bioavailability of fungal components after the particles are inhaled into the human lung. Due to their small size, fragments may be able to evade phagocytosis by macrophages, and can be translocated through systemic circulation.”
Subsequent research would advance on this study, such as Karunasena et al. (2010, Mycopathologia), which showed that damage to neurological cells from the mycotoxin Satratoxin H could occur at exposure levels found in water-damaged buildings.
***
We are only beginning to understand the spectrum of health effects related to exposure to dampness and mould. We still lack an understanding of predisposing genetics as to why some individuals in water-damaged buildings are adversely affected and not others. Despite many studies suggesting health effects as severe as neurological insults, directly showing dose-related effects following exposure has been difficult. The literature also contains animal studies that do show dose-related effects to exposure, with inherent limitations to translating to human effects. Synergistic effects from multiple microbes in a water-damaged environment as well as the specific effects of particular species on the central nervous system are poorly understood. Regardless of a full understanding of the mechanism to illness, a growing body of studies now indicate immune and neurological effects in predisposed individuals following chronic exposure to water-damaged buildings. Moreover, that exposure levels to such microbes can be high enough to cause chronic multiple-system inflammatory and immune effects is becoming increasingly understood.
For a more complete list of the science on this topic, please visit TMSA’s page on The Science of CIRS, which includes the Biotoxin Research Database—a curated list of peer-reviewed studies on this topic. Wikipedia also discusses the effects of dampness and mould on the innate immune system in humans.
PDF editions:

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment
You must be logged in to post a comment.