Public Hearing: On Thursday 9 August 2018 I attended an inquiry public hearing via teleconference. Other attendes included CIRS-aware doctors Sandeep Gupta and Mark Donohue, along with mainstream doctor Graeme Edwards. Building biologists Nicole Biljsma and Jeanette Williams, mycologist David Lark, IEP Jeremy Stamkos, Tenants union ACT also attended. You can download the the audio.
“Toxic Mould Support Australia, which I’ll refer to as TMSA, is a Facebook group that as of today has 3,312 members. It also has an associated website. The aim of the group and website is to raise awareness, and provide support to Australians suffering from health effects related to mould exposure. This includes the biotoxin illness Chronic Inflammatory Response Syndrome due to the environment of water-damaged buildings. Which I’ll refer to as CIRS from here on. This is a condition that I also suffer from.
Mold related illnesses, from mold allergy induced asthma to CIRS create a great burden of disease in Australia.
Daily, I hear the heartbreaking stories of those afflicted with chronic illnesses related to mould and see photos of terrible water damage to buildings. People write about how CIRS has devastated not only their health, but their relationships, their finances, and their faith in the medical, welfare and legal systems of this country.
I am here today to give voice to TMSA members, especially those who are not well enough to enter a submission to this inquiry.
Apart from the access to affordable medical care the issue of water-damaged buildings must also be addressed. There are fundamental issues with the design of buildings which includes the Australian building code, construction of buildings, their ongoing care and maintenance, and their remediation.
Patients struggle to find and afford healthy home and work accommodation. Landlords, real estate agents and insurance companies ignore their pleas for adequate remediation.
In summary, CIRS and other mold related conditions pose a significant public health and economic risk to Australia.
I look forward to discussing these issues with the committee roundtable session today.
Thank You.”
-
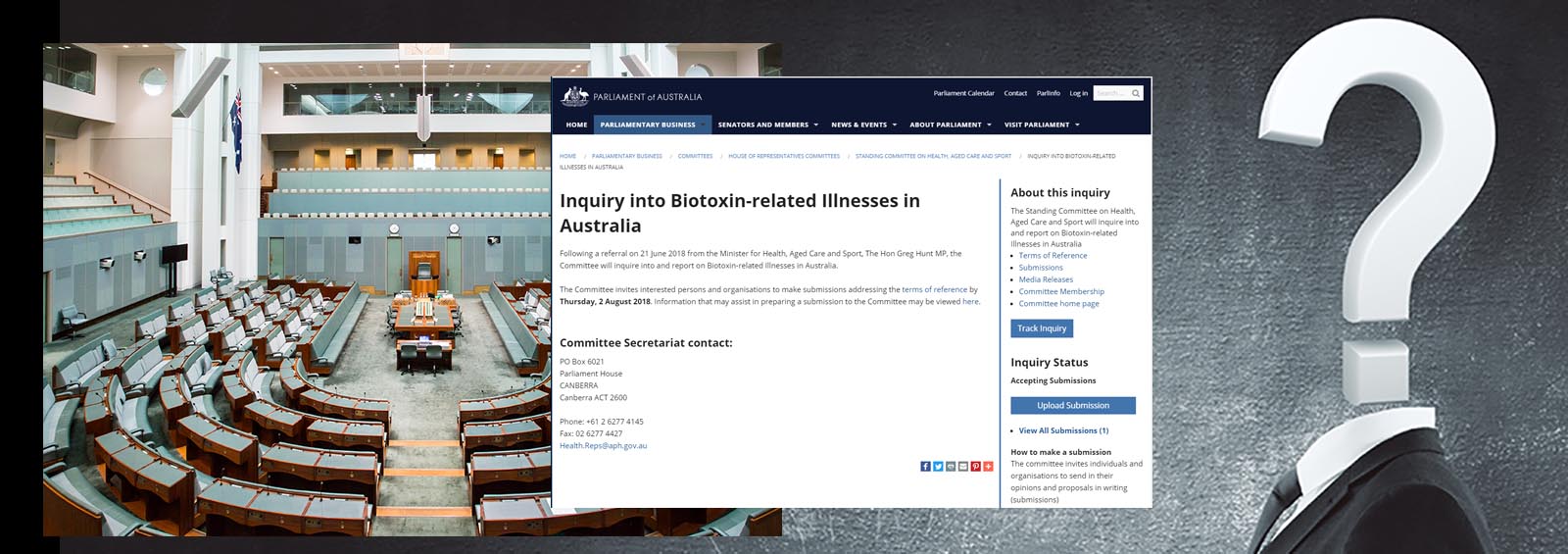
- Submission web page: Inquiry into Biotoxin-related illnesses in Australia
- Submission template: [DOWNLOAD] (Microsoft Word) (Thanks to Melinda Stephen)
- Submissions due date: Thursday, 2 August 2018
- Inquiry report due: by 21 October 2018
- The prevalence and geographic distribution of biotoxin-related illnesses in Australia, particularly related to water-damaged buildings;
- The prevalence of Chronic Inflammatory Response Syndrome (CIRS) or biotoxin related illness in Australian patients and the treatment available to them;
- The current medical process of identifying biotoxin-related illness in patients and the medical evaluation of symptom complexes attributed to biotoxins and CIRS;
- Any intersection with other chronic diseases;
- Investment in contemporary Australian research to discover and provide evidence of CIRS as a chronic, multisystem disease;
- Research into biotoxin-related illness caused from water damaged buildings; and
- Any related matters.
(From: Terms of reference web page)
- CIRS – Chronic Inflammatory Response Syndrome. A complex multi-symptom, multisystem illness due to the exposure of biotoxins, inflammagens and toxicants in the environment.
- WDB – water-damaged building(s).
- CIRS-WDB – Chronic Inflammatory Response Syndrome due to Water-Damaged Buildings. Also known as mould illness, sick building syndrome. Not mould allergy, which occurs due to IgE antibodies produced via the acquired immune system upon inhalation of mould spores, but rather an chronic activation of the innate immune system, its inflammatory proteins and gene dysregulation, due to exposure to biotoxins.
- CIRS-PLS – Chronic Inflammatory Response Syndrome – Post Lyme Syndrome aka Chronic Lyme disease. Borrelia spp bacteria and the parasite Babesia also produce biotoxins and can cause CIRS.
- Biotoxin illness – Illness caused by biotoxins and inflammagens found in water-damaged buildings, bacteria and parasite infection (Borrelia spp. aka Lyme disease, Babesisos), Ciguatera, toxic blue-green algae.
Points to consider (Medical)
- We need epidemiological studies to determine the prevalence in the Australian population. McMahon 2017 estimated the prevalence of CIRS to be between 7-12.7% in children and at least 7% in adults in two small clinical studies in New Mexico, United States. 7% of the Australian population would amount to 1.73 million people in total (24,770,700 total, ABS Dec 2017).
- Considering the possible prevalence of CIRS in the Australian population there is a vast shortage of general and specialist practitioners who are knowledgeable in the screening, diagnosis and treatment of the condition. Most health practitioners are only aware of mould allergy.
- Specialist general practitioners who are knowledgeable about CIRS, and their patients, should have access to MBS video consultation item numbers as many CIRS patients are bed and/or house bound or live substantial distances away from the small number of practitioners who treat CIRS.
- Chronic Inflammatory Response Syndrome (CIRS) should be a recognised medical illness throughout government departments, especially Centrelink, for disability pension and sickness allowance.
- Biotoxins and inflammagens found in water-damaged buildings are not limited to mould spores, but also fungal fragments, mycotoxins, mVOCS (microbial volatile organic compounds), VOCS from building materials, bacteria and bacterial toxins, viruses, parasites and more. Fungal fragments and toxins can persist even if mould is killed.
- Screening tools include visual contrast sensitivity testing (VCS) and symptom cluster analysis.
- Genetic susceptibility towards CIRS may be 24% of the general population (Dr. Shoemaker unpublished clinic data, Shoemaker et al, 2017)
- Accurate diagnostic biomarker testing is not available in Australia via a NATA/RCPA accredited laboratory for the following: Transforming growth factor beta 1 (TGB-b1), alpha-Melanocyte stimulating hormone (MSH), complement 3a (c3a), complement 4a (c4a), Matrix metallopeptidase 9 (MMP-9),and vascular endothelial growth factor (VEGF). These tests need to be a) available through common Australian pathology laboratories and have b) Medicare rebates available.
- Of those that are currently available some incur out of pocket costs (vasopressin/ADH, leptin). While for other accessible biomarkers (vasoactive intestinal peptide (VIP), estradiol, testosterone, serum osmolality, ACTH, cortisol, antigiladin antibodies, antiphospholipid antibodies) doctors are hesitant to request as bulk billed in case of Medicare audits.
- The primary medicine in the CIRS protocol, cholestyramine, is only available in Australia as Questran Lite (Aspen pharma care) that includes aspartame that many patients cannot tolerate. Most patients get the raw ingredient compounded without additives, leading to out of pocket costs.
- Secondary medicines; colloidal silver/EDTA nasal spray and VIP nasal spray are also compounded only medicines that also incur considerable out of pocket costs.
- CIRS and mycotoxins are linked to ME/CFS (Chester et al, 1994, Shoemaker et al, 2009, Gunn et al, 2016, Brewer et al, 2013), ulcerative colitis (Gunn et al, 2016), Alzheimer’s disease (Bredesen, 2016), Lyme disease (Shoemaker et al, 2008), Babesia (Shoemaker et al, 2006), Ciguatera (Ryan et al, 2015), Dinoflagellates/cynobacteria (toxic blue-green algae), (Shoemaker, 2001)
Points to consider (Water-damaged buildings)
- Problem of water-damaged buildings begins with the building code, design and building phases with increased energy efficiency leading to warmer, airtight buildings and non-awareness of vapour pressure management, causing condensation and mould growth even in new builds (Dewsbury et al, 2017). The recommendations of the Scoping Study of Condensation in Residential Buildings (Dewsbury et al, 2016) and the ABCB’s Condensation in buildings (2014) handbook need to be included into the Australian building code and made mandatory.
- Apart from design and construction issues water-damage can arise after construction due to natural events (storms, hail, cyclones and flooding), pipe and appliances leaks and occupant behaviour (cooking, drying clothes, overcrowding, overfilling of bath or sink etc).
- Indoor Environmental Professional (IEP) of building testing needs to be standardised and include professional visual inspection, moisture testing, VOC testing and testing of settled dust via qPCR (ERMI, HERTSMI-2) among other methods. Inspection and scope of works must be done by different parties than those doing remediation to negate conflict of interest issues.
- Mould remediation industry in Australia is unregulated with many remediators not following ANSI/IICRC S520 Mold Remediation industry standards. Many are using fogging, spraying and gassing in lieu of source removal which is advised against in the standard as it does not solve the problem and often makes it worse (see Medical talking points 2).
- Insurance, real estate and assessment industries often use mould testers and remediators based on lowest price and not to the above ANSI/IICRC standards.
- CIRS-WDB patients may need a higher mould remediation standard than ANSI/IICRC S520, see Schwartz et al. (2016). Indoor Environmental Professionals Panel of Surviving Mold – Consensus Statement.
- Based on percent of water-damaged buildings (see below) many private buildings – homes, work places, shops, restaurants – are not safe for those with CIRS-WDB.
- Likewise many public buildings are not safe for those with CIRS-WDB – schools, universities, public housing, armed forces quarters, prisons, law enforcement offices, emergency services offices, libraries etc.
- No Australian tenancy laws explicitly mention mould. Tenancy laws should adopt the recent Californian law that requires landlords to give written disclosure to prospective tenants when the landlord knows, or has reason to believe, that mold is present in the building that either exceeds the permissible exposure limits allowed or poses a health threat. The landlord has this responsibility when the mold is visible, invisible, or hidden (Legalmatch.com).
- The same should apply to residential and commercial building sales.
- Widespread awareness that killing mould with sprays (such as exit mould, vinegar and bleach) is not appropriate for anyone, especially for those with CIRS-WDB, rather prevention of moisture and then safe source removal of mould, is needed via public health initiatives.
References & Resources
Health effects of mould (CIRS-WDB specific)
See the CIRS Science page for a full list of peer reviewed papers and links to the full text. Significant peer-reviewed papers include:
- Shoemaker, R.C., Johnson, K., Lysander, J., Berry, Y., Dooley, M., Ryan, J. & McMahon, S. (2018). Diagnostic process for chronic inflammatory response syndrome (CIRS): A consensus statement report of the consensus committee of surviving mold. Internal medicine review, (6)5 May 2018. Full text
The most up-to-date paper on all types of CIRS by Dr. Shoemaker and his research team. - McMahon, S, Kundomal, K. & Yangalasetty, S. (2017). Pediatrics Norms for Visual Contrast Sensitivity Using an APT VCS Tester. Medical research archives, 5(5) May 2017. doi: 10.18103/mra.v5i5.1295 | Full text.
“Pediatric CIRS prevalence in this cohort was calculated as a minimum of 7.6% and a maximum of 12.7%. Pediatric CIRS prevalence is on the same order as pediatric asthma.” - McMahon, S. (2017). An Evaluation of Alternate Means to Diagnose Chronic Inflammatory Response Syndrome and Determine Prevalence. Medical research archives, 5(3), March 2017. doi: 10.18103/mra.v5i3.1125 | Full text
“At a prevalence of ≥ 7.01%, chronic inflammatory response syndrome is one of the greatest public health dilemmas in existence.” - Shoemaker, R.C., & House, D.E. (2006). Sick building syndrome (SBS) and exposure to water-damaged buildings: time series study, clinical trial and mechanisms. Neurotoxicology and teratology, 28(5), 573-88. PMID 17010568 | Full text
The (as yet) only double blinded randomized controlled trial into CIRS-WDB (then called Sick building syndrome) n=26 total, n=13 doubled blinded RCT wing. - Bredesen D.E. (2016). Inhalational Alzheimer’s disease: an unrecognized – and treatable – epidemic. Aging, 8(2), 304-13. doi: 10.18632/aging.100896 | PMID 26870879
Inhalational Alzheimer’s appears to be a subtype of CIRS. - Gunn, S.R., Gunn, G.G. & Mueller, F.W. (2016). Reversal of refractory ulcerative colitis and severe chronic fatigue syndrome symptoms arising from immune disturbance in an HLA-DR/DQ genetically susceptible individual with multiple biotoxin exposures. American journal of case reports, 2016(17), 320–325. doi: 10.12659/AJCR.896949 PMC491373
2 PMID 27165859
Health effects of mould on humans (not CIRS specific)
- Brewer, J., Hooper, D. & Muralidhar, S. (2015). Intranasal antifungal therapy in patients with chronic illness associated with mold and mycotoxins: an observational analysis. Global journal of medical research: K interdisciplinary, 15(1). Full text
- Brewer, J., Thrasher, J. & Hooper, D. (2013). Chronic illness associated with mold and mycotoxins: is naso-sinus fungal biofilm the culprit? Toxins, 24, 6(1), 66-80. doi: 10.3390/toxins6010066 PMID 24368325
- Brewer, J., Thrasher, J., Straus, D., Madison, R. & Hooper, D. (2013). Detection of mycotoxins in patients with chronic fatigue syndrome. Toxins, 11, 5(4), 605-17. doi: 10.3390/toxins5040605 PMID 23580077
- Campbell, A.W., Thrasher, J.D., Gray, M.R. & Vojandi, A. (2004). Mold and Mycotoxins: Effects on the Neurological and Immune Systems in Humans. Advances in applied microbiology, 55, 375-406. PMID 15350803, Full text
- Chester, A.C. & Levine, P.H. (1994). Concurrent sick building syndrome and chronic fatigue syndrome: epidemic neuromyasthenia revisited. Clinical infectious diseases, 18 Suppl 1:S43-8, PMID 8148452
- Gray, M., Thrasher, J., Crago, R., Madison, R., Arnold, L., Campbell, W. & Vojdani, A. (2003). Mixed mold mycotoxicosis: immunological changes in humans following exposure in water-damaged buildings. Archives of environmental health, 58(7), 410-420. PMID 15143854
- Morris, G., Berk, M., Walder, K. & Maes, M. (2015).The putative role of viruses, bacteria, and chronic fungal biotoxin exposure in the genesis of intractable fatigue accompanied by cognitive and physical disability. Molecular neurobiology. doi: 10.1007/s12035-015-9262-7 PMID 26081141, Full text
- Hope, J. (2013). A Review of the mechanism of injury and treatment approaches for illness resulting from exposure to water damaged buildings, mold, and mycotoxins. The scientific world journal, 2013. Full text
- Hooper, D., Bolton, V., Guilford, F. & Straus, D. (2009). Mycotoxin detection in human samples from patients exposed to environmental molds. International journal of molecular sciences, 10(4), 1465–75. doi: 10.3390/ijms10041465 PMID 19468319
- Ratnaseelan, A.M., Tsilioni, I. & Theoharides, T.C. (2018). Effects of Mycotoxins on Neuropsychiatric Symptoms and Immune Processes. Clin Ther. 2018 Jun;40(6):903-917. doi: 10.1016/j.clinthera.2018.05.004. PMID 29880330
- Thrasher, J.D. (2016). Fungi, bacteria, nano-particulates, mycotoxins and human health in water-damaged indoor environments. Journal of community and public health nursing 2016, 2(2). doi: dx.doi.org/10.4172/jcphn.1000115
Government / Other Organisations
- Global Indoor Health Network (GIHN) (2018). Diagnosis and treatment of illness caused by contaminants in water-damaged buildings. Link
The most up-to-date resource/paper of its kind, with many references that can be quoted. - World Health Organization (WHO) (2009). WHO Guidelines for Indoor Air Quality – Dampness and Mould. Link
- 10-50% of all indoor environments in Europe, North America, Australia, India and Japan are affected by indoor dampness; the numbers are much higher in some areas
- Microbial growth may result in greater numbers of spores, cell fragments, allergens, mycotoxins, endotoxins, β-glucans and volatile organic compounds in indoor air. The causative agents of adverse health effects have not been identified conclusively, but an excess level of any of these agents in the indoor environment is a potential health hazard.
- Well-designed, well-constructed, well-maintained building envelopes are critical to the prevention and control of excess moisture and microbial growth, as they prevent thermal bridges and the entry of liquid or vapour-phase water. Management of moisture requires proper control of temperatures and ventilation to avoid excess humidity, condensation on surfaces and excess moisture in materials. Ventilation should be distributed effectively throughout spaces, and stagnant air zones should be avoided.
- Building owners are responsible for providing a healthy workplace or living environment free of excess moisture and mould, by ensuring proper building construction and maintenance. The occupants are responsible for managing the use of water, heating, ventilation and appliances in a manner that does not lead to dampness and mould growth. Local recommendations for different climatic regions should be updated to control dampness-mediated microbial growth in buildings and to ensure desirable indoor air quality.
- Dampness and mould may be particularly prevalent in poorly maintained housing for low-income people. Remediation of the conditions that lead to adverse exposure should be given priority to prevent an additional contribution to poor health in populations who are already living with an increased burden of disease.
Papers about water-damaged buildings and building code
- Dewsbury, M., Law, T. (2017). Temperate climates, warmer houses and built fabric challenges. Procedia engineering, 180 (2017), 1065-1074. https://doi.org/10.1016/j.proeng.2017.04.266
“The recent enhancements of the National Construction Code have reduced the amount of energy required to heat and cool Australian homes. To date, the result of these changes, within Australia’s temperate and cool-temperate climates, is generally warmer internal temperatures. However, many of these warmer homes are presenting condensation and mould. This is demonstrating a general non-awareness of vapour pressure management within the Australian design and construction professions.” - Dewbury et al. (2016). Scoping study of condensation in residential buildings. Australian Buliding Codes Board. Retrieved November 14, 2017 from link and link [appendices].
- Shoemaker, R.C. & Lark, D. (2016). HERTSMI-2 and ERMI: Correlating Human Health Risk with Mold Specific qPCR in Water-Damaged Buildings. Proceedings of the 14th International Conference on Indoor Air Quality and Climate, International Society for Indoor Air Quality and Climate, Ghent, Belguim. Full text
- A large study of fungal DNA testing by MSQPCR using the HERTSMI-2 index of 807 buildings by Dr. Shoemaker and Australian mycologist David Lark (MouldLab). A safe HERTSMI-2 score for those with CIRS-WDB is < 10 (scale 0-50) with only 1.7-2.7% of patients relapsing. Patients will relapse 100% of time in buildings with a HERTSMI-2 of > 15 and 42-48% of time with scores between 11-14. Mean HERTSMI-2 of homes was 17.6, workplaces 15.5, schools 17.8.
Select Media Articles
- Atkinson, S. (2018, January 16). We can’t afford to ignore indoor air quality – our lives depend on it. The Conversation. Retrieved January 16, 2018 from link.
- Douwes, J. (2015, November 2). Health check: how does household mould affect your health? The Conversation. Retrieved December 14, 2015 from link.
- Katelaris, C. (2013, December 6). Queenslanders at risk from mould as flood clean-up continues. The Conversation. Retrieved December 14, 2015 from link.
- Zolfagharifard, E. (2014, December 19). Are energy efficient homes making us ill? Toxic mould caused by poor air circulation could trigger ‘sick building syndrome’. Daily Mail Australia. Retrieved December 14, 2015 from link.
- Full list


{kind=link}
{kind=link}
{kind=link}
{kind=link}