Mold, Lyme, fibromyalgia, chronic fatigue – when inflammation becomes chronic
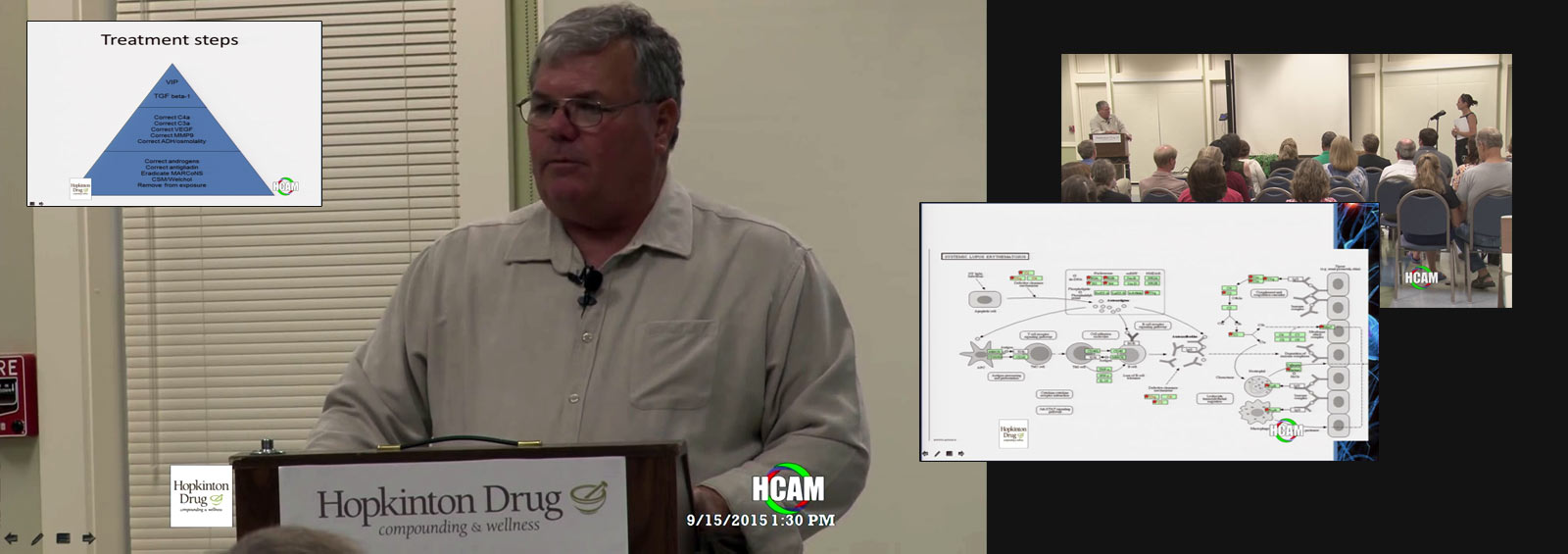
On 15 September 2015 Dr. Ritchie Shoemaker M.D. gave a nearly three hour lecture and question and answer session at Hopkinton Drug, a pharmacy who Dr. Shoemaker has collaborated with for two decades and which has provided many of the compounded medications (pure colestyramine, BEG spray, VIP spray) necessary for his treatment protocol. In this lecture Dr. Shoemaker details the major players in chronic inflammatory response syndrome due to water damaged buildings (CIRS-WDB, aka. mould illness) and post Lyme syndrome, talks about his forthcoming genomics paper, NeuroQuant, Pfiesteria, ERMI, HERTSMI-2 and has an in-depth Q&A where he questions the diagnosis of several tick borne illness patients, discusses the problems with Realtime Labs urine mycotoxin testing and much more.
Jump to
Dr. Shoemaker Lecture (Slides denoted by square brackets)
- 0:00:42. Introduction (Dennis Katz and Terry from Hopkinton Drug)
Relationship with Dr. Shoemaker started in 1993 with compounded CSM. 50 people behind the scenes of Hopkinton - 0:03:50. Ritchie Shoemaker, M.D.
- 0:06:25. “If you think this illness is not real, I’ve only treated 7,000 [mold] patients. 2,000 Lyme patients and about 1,000 ciguatera/dinoflagellates. “
- 0:06:50. We have finished the last bits and pieces on our paper on genomics. Within a short period of time you will be able to read about the gene activation that is abnormal as a fingerprint in people who have been exposed to water damaged buildings.
- 0:07:30. Genomics and cancer. 25,000 protein coding genes, 25,000 genes were thought to be junk DNA, instead are regulatory genes.
- 0:08:15. When you see someone with post-Lyme syndrome being treated with antibiotics and nothing for the genomic basis of their illness, they won’t get better. When someone moves out of a moldy building into a brand new building, that’s not guaranteed to fix their illness. Now we know the gene abnormalities and even better have treatment. Tonight I’ll show you how to shut off the 2,000 protein and non-protein encoding genes that are a part of this.
- 0:11:22. “When I say mold I mean people who are ill from water damaged buildings. Is it just mold? Mycotoxins? Hardly. Mycotoxins are very small part of this illness. We’re talking about bacteria and bacterial toxins. Actinomyces and actinomyces toxins. Talking about breakdown products of whole cells called fragments which aren’t alive. They’re dead. They’re chemicals”
- 0:12:00. If someone tells you they’ve fixed your home or school by fogging with some magical liquid that kills things – say “I’m glad you can kill 0.01% of the problem. I’d like you to remove 99.9% of the actual problem.”
- 0:12:30. Bacterial sepsis (Systemic Inflammatory Response Syndrome SIRS). Bacteria in bloodstream doesn’t make people sick but overreaction of the immune system of the host response. SIRS was the origin of CIRS.
- 0:14:13. [CIRS]. Cytokines . C3a (up in Lyme), C4a (up in mold and Lyme)
- TGF-b1. Major player. Affects fibrosis, changes in lungs, affects cells types. Turns on differential cell activation. Five years ago there was 75,000 references in peer reviewed literature. Type 2 diabetes had 81,000.
- 0:16:28. Von Willebrand’s. More people with acquired Von Willebrands syndrome in this room than we’re likely to find in the rest of Boston put together. C4a causes it, VIP fixes it.
- Asked Dennis in 2005 about making VIP. Had it in 2008. Is it a miracle drug – yes. 2,000 people on it and four drop outs.
- 18:30. [Goals for today]
- NeuroQuant (NQ) – Is an FDA cleared program, since 2006, costs $89. It gives you 11 different areas of the brain and incredible detail of structure and size. Creates a fingerprint which I can look at and recognize in about in ten seconds that says mold. Atrophy, memory problems. Protocol fixes three of the main elements, VIP fixes the last – caudate atrophy. If you have loss of substance in the brain from Alzheimer’s is there anyone ever that has shown regrowth of brain tissue once atrophied? NQ tells us that VIP does that.
- 0:20:10. [But there is more…]
- One person does make a difference.
- [If you already know CIRS]
- CIRS is typified by genetic susceptibility. Typified by lack of control of inflammation due to low MSH and VIP (usually deficient before other labs).
- We know more about the genome and CIRS than anybody know about the human genome and cancer or atherosclerosis. Why? Because we have a way to treat the illness.
- 0:23:40. [Biotoxin pathway]
- “Innate immune system designed to detect invasion from foreign antigens and deal with antigens by setting off exponentially expanding cascade of inflammatory response. Why? Antigens need to be removed when they’re not us. Defect in this illness is antigen detection mechanism works, sets off the inflammatory response, shuts down MSH and VIP, but does not result in antibody formation that clears the antigen”.
- If you leave a moldy building does the antigen leave you? No, it stays. Worse it recruits new genes to be involved, new abnormalities to be involved.
- 0:25:55. So many effects of cytokines. MSH deficiency knocks out ACTH and cortisol regulation. Adrenal fatigue patients – did anyone measure MSH which controls ACTH and cortisol before you poisoned that pathway with cortisol replacement? Same with androgens (testosterone cream).
- 0:28:00. Antidiuretic Hormone (ADH), linked to MSH. Static shocks. Sweat chloride levels higher than cystic fibrosis patients. ADH will be low and osmolality sky high. Headaches that act like migraines. Common in younger women, especially tall and slender (11-3-52Bs). Stand up and blood pressure starts to fall, rapid heart rate, not POTS, instead pulmonary hypertension and dehydration from MSH deficiency.
- 2006 Senate talk and St. Bernard’s parish report and cover up. NIOSH didn’t sample any of the WDBs for mold despite visually seeing it.
- 0:33:10. [Complement and coagulation cascades]
- Any gene pathway that was abnormal before VIP (green) are corrected by VIP (green with star)
- 0:34:37. [If you don’t know] [Am I talking about a small, obscure problem?]
- NIOSH says 50% of buildings are WDB. Likely more.
- 0:36:00 – “If you have to leave your house, if you have to leave your workplace – because that’s the first thing we tell people to do, get out of exposure – where are you gonna go? Wintertime’s coming you can’t go in a tent in the backyard for very long and you won’t get any better moving to Arizona unless you’re in that tent because wherever there’s indoor water, wherever there’s plumbing, wherever there’s a roof, they’ll be water intrusion. If the water intrusion is there for two days you’ll have mold, bacteria, actinomyces and all the inflammagens.”
- 0:37:20. [Tick bites]
- Tick borne infections are: Under-diagnosed – show me a reliable test for Bartonella.
- And: Over diagnosed. Only one case of Babesia in Maryland (Gibson Island) yet everyone shows their positive Babesia labs. Yeah sure you do. Who did your smear? Who measured your haptoglobins? Who looked for intravascular hemolysis? Who showed hemoglobin urate?
- Dropped out of ILADS group in 2002, drove me nuts. I’ll fight anybody if I think they’re wrong.
- Post-Lyme is CIRS. Just collect the labs. Just Lyme protect you from mold? No. Do symptoms of Lyme and mold overlap about 100%? Yes. How do you separate? Do a C3a (Quest, not Labcorp), do a NeuroQuant, do genomics test (not available commercially yet).
- 0:40:00. [Cyanobacteria]
- Ipswich river
- 0:40:50. [Each of these categories of illness can be acute and chronic]
- Once you’ve been sick with these illness for a month or two, we have a final common pathway. All of these start to have same symptoms, VCS abnormalities and labs.
- 0:41:05. [Fingerprints everywhere]
- Fingerprints galore now. NQ: Swelling on a microscopic basis in at least three nuclei (forebrain, cortical gray, pallidum). Caudate atrophy – mold patient. Interstitial edema of the thalamus and putamen atrophy? That’s a Lyme patient. How about PTSD? They’ve all got small hippocampi. Important to look at PTSD as an inflammatory disease, not psychiatric.
- 0:42:20. [First day of med school] Acute inflammation, finger analogy.
- What makes or sepsis survivor have cognitive issues a month after the ICU? Inflammatory response syndromes are not unusual, happen all the time. In molecular biology you don’t always get warmth, redness, pain and swelling.
- 0:44:00. [Response to injury? What?]
- 0:44:15. [Molecular biology] Simple model of double helix doesn’t apply anymore, what about microRNA and mRNA. Every microRNA will police 10-100 mRNAs. Regulation of gene activity post-hoc, after transcription. We have regulation (microRNA) of regulation (mRNA) of DNA transcription (DNA).
- 0:47:20. [Substitute chocolate for inflammation] Chocolate analogy
- 0:48:28. [What if chocolate caused an illness?] [And even worse]
- 0:50:45. [So this guy walks into a cancer ward] Talks about his time going to hematology office, located in oncology, and people labelling him with cancer.
- 0:51:34. [When people don’t look ill, can they be disabled and hurting?]
- But what about a mold patient? Chronic fatigue, chronic pain, IBS, memory, numbness, tingling, Parkinson’s.
- 0:54:30. [Leprosy? I thought this talk was about mold and Lyme]
- How many people in your quest asked you if it was a psychiatric illness? All of them.
- 0:55:48. [What about an exposure history?]
- 0:56:50. [Lyme? Post-Lyme] If you’ve got Lyme and are being treated with antibiotics you need to know if you’re being exposed to mold or not. HERTSMI-2 from Mycometrics costs $125. Collect dust, they look for mold DNA, in two areas of your home (master bedroom and living room). Swiffer cloth or vacuum attachment if you have carpets.
- 0:57:55. [But the nagging doubt] 2007 study from EPA, 21% of asthma caused by WDB. Truth is that most asthma is restrictive, not obstructive, lung disease. Called asthma incorrectly. But if you look at markers in restrictive lung disease, TGF-b1, C4a, MMP-9, VEGF, jump off page. Throw away the asthma diagnosis when you fix the patient.
- 0:58:50. [CIRS, a brief history]
- 0:59:40. MARCoNS, a commensal organism, causes no symptoms in low MSH patients. May be in the gut too, we don’t know. They make compounds which are genomically active, changes gene activation.
- 1:00:40. [CIRS is systemic, interacting]
- 1:01:24. [Innate immune effects are systemic. Everywhere blood goes…] Treg cells C4+/CD25++, stop autoimmunity in tissues under direction of TGF-b1. If no ROR they get converted into more TGF-b1.
- Collaborated with two TV shows CSI Cyber season 1 episode 10 “Click Your Poison”. Also Monsters Inside Me, season 6 episode 4 “There’s a Fungus in My What!?!” (airs 4 November 2015).
- 1:04:45. [CIRS. Some history begins an anomaly: the illness was real] Talks about beginning when prescribing CSM to a pfiesteria patient to fix secretory diarrhea, which fixed her other symptoms (headache, memory, cough). CDCs attitude to CSM therapy “premature.”
- Need to read State of the art answers to 500 mold questions. Stick with the science. Stick with what’s peer reviewed.
- 1:11:25. [Multisystem, multi-symptom illness all happened at once] Couldn’t figure out why some got sick and some didn’t in initial Pfiesteria clusters.
- 1:12:10. [Easy to look back and say “of course we see the problem”]
- 1:12:18. [More people become ill] [Picture of lesions]
- 1:13:58. [What did the kills tell us] [Porewater] [Blue mold starts in NC] [Curious coincidence] [The copper theory arises]
- 1:15:22. [Vegetation changes in estuaries map]
- 1:15:40. [The lessons of Pfiesteria repeat]
- 1:15:40. Principles of ecology of WDB similar to Pfiesteria. Two days of water intrusion leads to microbial growth.
- 1:16:28. [Labeled for reducing cholesterol] CSM treatment. Pfiesteria was from breathing bio aerosols not eating the fish. Same analogy goes with WDB. “Any food will give you mycotoxins in the urine, big time. That’s why doing testing the urine for mycotoxins I don’t think is a great idea. Some people like it, I don’t. Why? You just told me what I had to eat last month.”
- 1:17:08. “CSM works by having its positive charge on a side chain and binds to these biotoxins which have negative charge in their linkages. And it prevents this negative charged tiny compound from being reabsorbed.”
- 1:17:45. Dennis created MCS version of CSM in a couple of days. Invented BEG spray within a couple of weeks. Created VIP. Used by Shoemaker himself (thanksgiving 2008, building fences)
- 1:19:36. [Figure 1: binding of ammonium cation]
- 1:20:05. [Ciguatoxin chemical structure] [Other toxins]
- Look at all the double bonded oxygen molecules. CSM fits right in there and binds it.
- 1:20:48. [Ochratoxin A] [Toxin table] [200 Pfiesteria people get better…] [Types of Toxic Cyanobacteria] [Current Study – St. John’s River]
- 1:21:30. [Symptoms & Biomarkers of Effect] [1998 first mold patient] [WDB photo] [Defining mold illness]
- 1:22:14 (Slides zoomed past)
[Say it in a lot of words] [Genetics of inflammatory illness] [What is a “moldy” building?] [HERTSMI-2] [Case definition-1] [Case definition-2] [Who gets sick?] [HLA Disequilibrium] [1999 Lyme toxin patented] [Is the Lyme cytokine profile different from that of mold and others?] [Genomics-3] - [SLE pathway] Abnormal genes in lupus treated successfully with VIP
- 1:23:10. [Cytokine Receptor Interaction]
In 1985 there used to be just a few of them. First paper on TNF. [Cell Cycle] - 1:23:44. Looking at mold illness/CIRS as markers as markers of a brand new era of treating inflammatory diseases of the 21st
- [Summing up] Follow the data. Don’t make assumptions. [Follow the data!]
[Treatment steps] Goes through pyramid. - 1:27:24. “VIP is like a coat of paint. If a body with inflammation is burning you don’t try to paint it. It won’t work. But if you put out the fire and then you put the coat of paint on now it will work. VIP is your coat of paint. Fixes proteomics, fixes the brain, fixes genome.”
- survivingmold.com
Questions and Answers (click to reveal answer)
- 2:45:20. Closing (Dennis Katz)
- 2:46:30. End.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment
You must be logged in to post a comment.